Corynebacterium Diphtheria
Corynebacteria are one of the gram positive bacteria which is non acid fast, nonmotile rods with irregularly stained segments and sometimes granules. Term corynebacterium given to them because they frequently show club shaped swellings.
Corynebacterium diphtheria, is one the most important member of its genus. It the causative agent of diphtheria.

Morphology
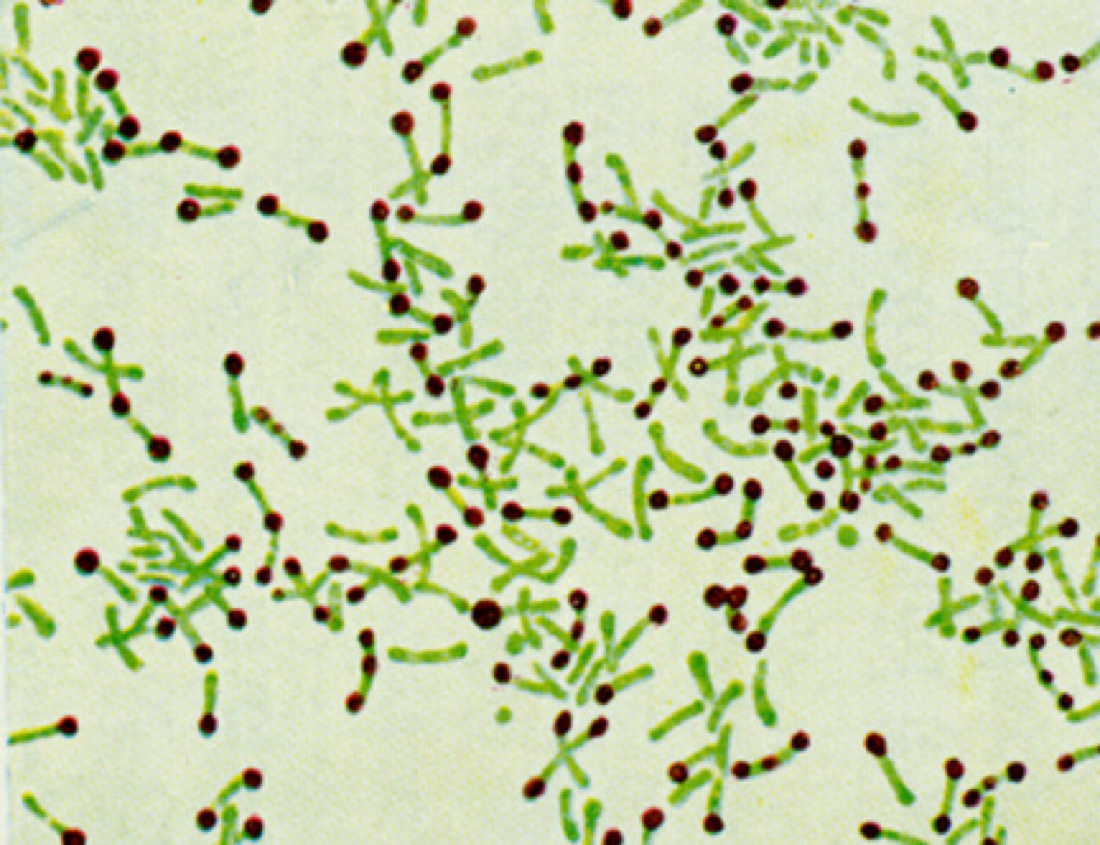
Beside showing all the property of Corynebacterium, diphtheria bacillus is a slender rod with a tendency to clubbing at one or both ends, its size is approximately 3 – 6 micro meter X 0.6 – 0.8 micrometer. Diphtheria bacilli are pleomorphic. They are non sporing, non capsulated and non motile. Its cells often show septa, and branching. These are gram positive but having a tendency to be decolonized easily. Diphtheria bacilli have granules those are composed of polymetaphosphate are seen in the cells.
Cultural Characteristics
On ordinary media, diphtheria bacilli show scanty growth. Enrichment with blood, serum or egg is necessary for good growth. The optimum temperature for growth is 37 C (range 15 – 40 C) and optimum pH 7.2. it is an aerobe and a facultative anaerobe.
Diphtheria bacilli very rapidly grow on Loeffler’s serum slop and colonies can be seen in 6 – 8 hours, long before other bacteria grow. Its colonies are at first small, circular white opaque discs but enlarge on continued incubation and may acquire a distinct yellow tint.
Biochemical Tests
Diphtheria bacilli ferment with the production of acid, (but no gas) glucose, galactose, maltose and dextrin (but not lactose, mannitol or sucrose). Some strains of virulent diphtheria bacilli have been found to ferment sucrose. It is necessary to employ Hiss’s serum water for testing sugar fermentation. Proteolytic activity is absent. They do not hydrolysis urea or form phosphatase.


Toxin
A very powerful exotoxin is produced by virulent strains of diphtheria bacilli. The pathogenic effects of the bacillus are due to the toxin. Almost all strains of gravis and intermedium’s (about 95 – 99%) are toxigenic, while only about 80 – 85% of the minis strains are so.
There is the considerable variation in the amount of toxins produced by different strains, some strains producing it abundantly and others only poorly.
‘Park Williams 8’ strain is used for toxin production, almost universally.
Diphtheria toxin is a protein and has been crystallized. Its molecular weight is about 62,000. It is extremely potent and the lethal dose for a 250 g guinea pig is 0.0001 mg. it consists of two fragments, A and B, of MW 24,000 and 38,000, respectively. Both fragment of this protein is necessary for the toxic effect.
When released by bacterium, the toxin is inactive because the active site on fragment A is masked. Activation is probably accomplished by proteases present in the culture medium and infected tissues.
All the enzymatic activity of the toxin is present in fragment A. fragment B is responsible for binding the toxin to the cells.
The toxin is labile. Prolonged storage, incubation at 37 C for 4 – 6 weeks, treatment with 0.2 – 0.4 % or acid pH converts it to toxoid. Toxoid is toxin that has lost its toxicity but not its antigenicity.
Resistance
Cultures of diphtheria may remain viable for two or more weeks at 25 – 30 C. it is readily destroyed by heat in 10 minutes at 58 C and in a minute at 100 C.
It is more resistant to the action of light, desiccation and freezing than most non sporing bacilli.
It remain fully virulent in blankets and floor dust for five weeks. It is easily destroyed by antiseptics. It is susceptible to penicillin, erythromycin and broad spectrum antibiotics.
Pathogenicity
The incubation period in diphtheria is commonly 3 – 4 days but on occasion be as short as one day. In carriers, the incubation period may be very prolonged. The site of infection may be faucial, laryngeal, nasal, otitic, conjunctival, genital-vulval, vaginal or prepucial and cutaneous.
Treatment
Specific treatment of diphtheria consists of anti toxic and antibiotic therapy. Antitoxin should be given immediately when case is suspected as diphtheria.
Corynebacterium diphtheria is sensitive to penicillin and can be cleared from the throat within a few days by penicillin treatment. Diphtheria patients are given a course of penicillin though it only supplements and does not replace antitoxin therapy. Erythromycin is more active than penicillin in the treatment of carriers.
Reference: Text Book Of Microbiology


