Neisseria Gonorrhoeae (Gonococcus)
N. gonorrhoeae causes the venereal disease gonorrhea. This gonococcus was first described by Neisser in 1879 in gonorrhea pus. Its culture and pathogenicity was first described by Bumm in 1885. Gonococci and meningococci are very close in many properties.
Morphology
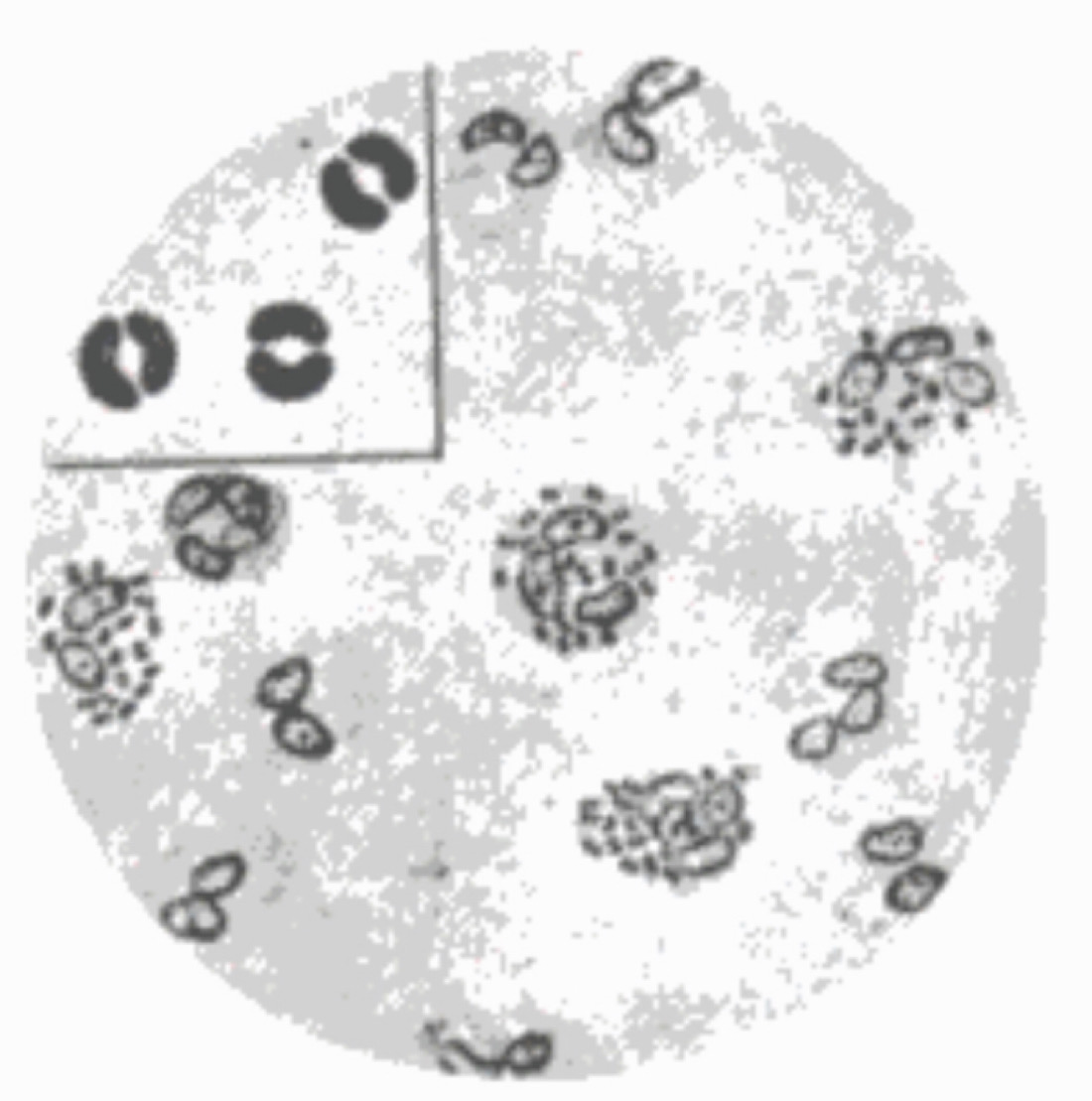
In acute gonorrhea, smears formed from urethral discharge, the organism appears as a diplococcus with the adjacent sides concave, like kidney – shaped.
Gonococci possess pili on their surface. These pili facilitate gonococci to adhere on mucosal surface and promote virulence by inhibiting phagocytosis. These pixilated gonococci agglutinate human red blood cells, but this feature is not shown in other mammals.
Cultural Characteristics
If we compare it with meningococci, gonococci are more difficult to grow on artificial media. They are aerobic but may grow anaerobically also. Growth occurs best at pH 7.2 – 7.6 and at a temperature of 35 – 36 C. 5 – 10% CO2 is essential for its growth. Mueller – Hinton agar and chocolate agar shows its good growth. A popular selective medium is the Thayer – Martin medium (containing vancomycin, coli stain and nystatin) which inhibits most contaminants including non pathogenic neisseria.
Once grown on artificial media, gonococci colonies are small, round, translucent, convex or slightly umbonate, with finely granular surface and locate margins. They are soft and easily emulsified.
Biochemical Reactions
Meningococci and gonococci show similar set of biochemical reactions except in the effect of maltose. as gonococci acidify only glucose and not maltose.
Gonococci contain several plasmids. However, its 95% of strains have a small cryptic plasmid of unknown function. Other two transmissible plasmids contains genes those code for beta lactamase which causes resistance to penicillin.
Epidemiology
Gonorrhea is an exclusively human disease. However, experimental disease may be produced in chimpanzees by urethral inoculation.
The only source of infection is a human carrier. The existence of asymptomatic carriage in women makes them a reservoir. The mode of infection is almost exclusively venereal.
Laboratory Diagnosis
In acute gonorrhea the urethral discharge contains gonococci in large numbers. In women, besides the urethral discharge, cervical swabs should also be collected.
In chronic infection, there may not be any urethral discharge.
For culture, specimens should be inoculated on prewarmed plates, immediately on collection. If this is not possible, specimens should be collected with charcoal impregnated swabs.
In acute gonorrhea, cultures can be obtained readily on chocolate agar or Mueller – Hinton agar incubated at 35 – 36 C under 5 – 10% CO2. In chronic cases, it is better to use a selective medium such as the Thayer – Martin medium. The growth can be identified by morphology and biochemical reactions.
Treatment
In 1935, when sulphonamides were interdicted for the treatment of gonorrhea, all strains were sensitive to the drug but resistance developed rapidly. When penicillin was introduced, all strains were highly sensitive. From 1957, strains with decreased susceptibility become common.



